- Joined
- Jul 26, 2007
- Messages
- 12,692
- Reaction score
- 2,311
Sounds great in theory when your show them that models and pictures etc. No data needed!
Are we talking about protons or spaceoar?

Sounds great in theory when your show them that models and pictures etc. No data needed!
Could work for either! The irony of course being they are often used togetherAre we talking about protons or spaceoar?
Is that a falafel gyro in B?
If you're getting an MRI after SpaceOAR Vue because you can't trust you didn't infiltrate rectal wall you should just stop placing the SpaceOAR, IMO.These reports make me soooo nervous.
I still offer spaceOAR but certainly don't push it. I'd say about 30% of my prostates get it. It is very prevalent in my community, so patients are asking for it/about it.
I know the VUE can be seen on CT but I think it's VERY important to get a post insertion MRI - it will show rectal wall infiltration much better. I don't offer spaceOAR to anyone that can't have an MRI.
I then carefully look at it and review with our prostate MRI folks. If any rectal wall infiltration they need to do a proctoscope and look at mucosa. If any mucosal alteration then you need to wait and not start radiation. I am convinced spaceOAR bad placement plus SBRT is a PROBLEM. If any concern at all about placement then I think they need switched to 28+ fractions.
Here is a study that "suggests" due to the increased toxicities of hypofractionation that SPACEOAR/BARRIGEL should be utilized. I thought the toxicity of hypofractionation wasn't higher than conventional radiotherapy?

Hyaluronic Acid Spacer for Hypofractionated Prostate Radiation Therapy
This randomized clinical trial examines whether a hyaluronic acid rectal spacer could improve rectal dosimetry and affect acute grade 2 or higher gastrointestinal toxic effects for hypofractionated radiation therapy.jamanetwork.com
Prepare for silence or "I've never seen this in my clinic."
I have seen rectal wall infiltration in two cases, neither of whom I did their spaceOAR. I'm certainly not claiming I'm an expert on it. Probably a denominator at this point of ?50? . Fortunately they both have turned out fine.
I reached out to a lot of experts and got a lot of opinions. For anonymity I'll decline to say who I communicated with. Consensus was get a look at mucosa before doing anything. If mucosa intact and no symptoms and you really want to start then switch away from SBRT and do 28+. If mucosa issues then do not start treatment. Wait until it completely clears up and re-image before doing anything radiation wise.
Aside - at least in my training years ago the reps will tell you to "push through the rectal hump" to get in the space. I am confident many times the needle goes through mucosa then back out of mucosa and into the space. It's mostly fine, but when it's not fine it's a problem. A BIG problem.
The seminal published trial is ALL conventional Fx. There is an ongoing SBRT +/- Spacer trial.It's been a while since I've read the studies...
Did all of the patients on the randomized trials have post-spaceOAR MRI's?
Also I wonder what % of these MAUD cases are SBRT versus hypo or standard frac?
Looks like there have also been at least 3 deaths resulting from MI immediately after placement. Seems that these were done with local. Very alarming.
View attachment 375956
SBRT up to 40 Gy in 5 fx is perfectly safe without any gel whatsoever.
I always make sure patients understand that people are paid to place the device, and that payment is what is driving usage, which I very truly believe. The data show- unequivocally- that placement of the device results in 100% grade 2 toxicity and does not substantially reduce long-term grade 2 or 3 toxicity. The data via MAUDE have also shown several grade 5 toxicities. How many grade 5 toxicities are acceptable? I would argue the number is zero.
One and the same!Are we talking about protons or spaceoar?
If you're getting an MRI after SpaceOAR Vue because you can't trust you didn't infiltrate rectal wall you should just stop placing the SpaceOAR, IMO.
Good post!If you're getting an MRI after SpaceOAR Vue because you can't trust you didn't infiltrate rectal wall you should just stop placing the SpaceOAR, IMO.
Every SINGLE prostate mod hypofrac trial shows increase in acute GI toxicity compared to conventional. This is also reflected in ASTRO moderate hypofrac guidelines. Not surprising spaceOAR could reduce acute GI toxicity. As others have stated, placing a needle into the perineum is immediately at least a G2, if not G3, acute toxicity.
Part of the reason they allow you to do it is because they tell you never to pullb ack on the needle while you're injecting. Hold the needle in the position you have it once you finish injecting for a little bit to let gel solidify before you retract needle (and pull some of the gel through the rectal hump potentially.
BUT - I would not recommend putting a needle through the rectal hump if you can avoid it. Come in at an angle over it and then angle down once you're past the hump.The needle is flexible and with good TRUS guidance you can angle it. Make sure you're not coming in too low/flat at the skin that you have to go UP over the hump and then back down after the hump - not sure how the needle feels about holding an inverted U-shape.
The seminal published trial is ALL conventional Fx. There is an ongoing SBRT +/- Spacer trial.
C'mon man, how a spacer gel going to cause a MI? Even a vascular embolus isn't going to be an MI.
Published data on dose escalating like that? Meeting V38 < 2cc for rectum would be VERY difficult for most of my patients when doing 40/5 without a gel.
Don't disagree with the rest.
I'm not a die hard supporter but I think some of this is sensationalism and a fair amount of it is likely people not taking the time to do it safely. I'm not an expert in it and like having the rep there every case. Ortho bros can do it with Stryker, why not with these other reps?
If no VUE then yes post spaceOAR MRI is mandatory (and part of the reason it's stupid, IMO).the urologists don't have VUE (or aren't placing it yet). I *think* they bought a bunch of regular spaceOAR and are working their way through the supply.
So I get MRI for planning and for visualization.
With that said, in the limited VUE cases I've seen, I still feel best about a no-charge post insertion MRI. I just do a thin cut T2 small field of view axial and saggital on same day as ct sim.
If you do an MRI aren't you required by law to charge it?
Same true w/mri for cervical hdrMy MRI dept is very friendly and we have a spaceOAR protocol MRI and they no-charge it. The scan is very quick and there's no prep like rectal contrast, IV contrast, etc.
You don't get paid for say an MRI for a gamma knife on day of GK (bundled into treatment) or a few days before GK (the new ICON can use non-frame MRI imaging...we often get a new MRI day before GK for mets cases and no-charge it especially if they had a diagnostic pre-steroid MRI a week or so prior), so I see no reason that it's mandated to charge for an MRI if I get a quick scan and don't get a radiology read on it.
C'mon man, how a spacer gel going to cause a MI? Even a vascular embolus isn't going to be an MI.
Not sure but posted because all of these events happened immediately after placement (don't think any had sedation/ general). It looks like 90/120-day mortality has been assessed after prostate biopsy but could not find anything on immediate serious events as a comparison. While very rare, would prefer to avoid running a code in clinic at all costs.
1.
It was reported that minutes after finishing the procedure, the patient suffered from a "heart attack". This was further clarified as the patient "started to get very red in the face, arching back, got very stiff" but he was still talking and stated that he was "ok but seemed to be having a bad back spasm". The patient started turning blue and pulse oximetry showed his oxygen saturation was dropping. The patient was started on 10l of oxygen and stopped responding verbally.
2.
After the procedure was discontinued, the rectal ultrasound probe was removed from the patient's rectum. A few seconds after the rectal ultrasound probe was removed, the patient said that he was nauseous and began to vomit. The patient experienced a syncopal event. Additional nursing staff was called to assist the patient, because it was believed he was experiencing a vasovagal response. The patient became unresponsive, and a code blue was called. Additionally, emergency services were called. The patient was administered oxygen, fluids, and cpr for 45 minutes. The patient was then transferred to the emergency department (ed).
3.
After the injection of the hydrogel the stepper probe was removed, the patients' legs were lowered, and the patient was instructed to stay laying down to avoid being lightheaded. After 10-15 seconds the patient said that he was lightheaded. Ten (10) seconds later the patient rolled to his side and attempt to vomit, dry heaved, then the patient laid back down and said he wasn't feeling ok. The patient dried heaved again and laid down. The patient was cyanotic, and lost consciousness. It was reported the patient was breathing but was not responsive, rapid response turned into code blue, the patient was intubated and was injected with epinephrine and sodium bicarbonate. Cardiopulmonary resuscitation was performed for 20 minutes and since there was no shockable rhythm the patient was never shocked. The patient was then pronounced dead. An autopsy was performed and reported the cause of death as natural causes due to hypertensive atherosclerotic cardiac disease.
Pudendal nerve stimulation can cause autonomic dysfunction. In a man with marginal cardiovascular health, this could do the trick.Vasovagal events are not uncommon with pelvic procedures.
Might not have known the patient was a heart attack waiting to happen...Pudendal nerve stimulation can cause autonomic dysfunction. In a man with marginal cardiovascular health, this could do the trick.
Of course, the cardiovascularly frail usually don't need prostate treatment.
Glass half empty . . . think of the time that the patient will save by pooping and peeing at the same time! Only half the trips to the bathroom!
So in my personal sphere, I know for a fact it's significantly diminished. There's one doc left doing it routinely...and he's imminently retiring. The practice patterns in my area are a little strange in a way where I don't put a lot of weight behind this statement, but I haven't had many patients asking about it this year.spaceOAR is very depressing. I wonder if it’s on its way out already. Doing it in 2023 is like going to Burning Man
Do you mean in your own cases, or in cases you see from your colleagues?Barrigel is better IMO.
Sounds like it’s not a popular opinion around here, but I’ve DEFINITELY noticed a reduction in GI toxicity since using hydrogel. Every single time in the past 3 years that someone has any significant or lingering GI toxicity, they didn’t get hydrogel.
Do you mean in your own cases, or in cases you see from your colleagues?
My personal observation: with RadOncs who attempt an optimal sim/treatment setup, minimizing rectal filling, contour and expand according to consensus guidelines, keep rectal constraints within standard modern limits, daily CBCT with therapists who will watch rectal filling and compensate accordingly - no benefit to GI tox.
With RadOncs who lack formal training in VMAT-era/OBI technologies and contouring, who are less attuned to QUANTEC constraints and don't emphasize to the therapists the importance of certain things in daily IGRT...
Hydrogel spacers seem helpful for those doctors.
Do you mean in your own cases, or in cases you see from your colleagues?
My personal observation: with RadOncs who attempt an optimal sim/treatment setup, minimizing rectal filling, contour and expand according to consensus guidelines, keep rectal constraints within standard modern limits, daily CBCT with therapists who will watch rectal filling and compensate accordingly - no benefit to GI tox.
With RadOncs who lack formal training in VMAT-era/OBI technologies and contouring, who are less attuned to QUANTEC constraints and don't emphasize to the therapists the importance of certain things in daily IGRT...
Hydrogel spacers seem helpful for those doctors.
Are we talking about protons or spaceoar?
I know I'm not ese, but we put patients on a bisacodyl regimen and back off as needed. Keeps things small and consistentI'm curious for your tips on the bolded. Most of what I've seen don't recommend any specific rectal interventions in the era of CBCTs.
You tend to have super well thought out tips, so figured I'd ask 😊
Hahahaha I know I was trying to word it in a way where it didn't force you (or anyone else) into a defensive corner because that's not my intent.Well, based on the rest of what you’ve said, this is a loaded question.
I can only speak for my patients, but I definitely feel (subjectively) like it helps. At 3 months after treatment, virtually no one has any residual GI issues unless they didn’t get the gel.
I'm curious for your tips on the bolded. Most of what I've seen don't recommend any specific rectal interventions in the era of CBCTs.
You tend to have super well thought out tips, so figured I'd ask 😊
Here's the issue. Go back and watch the prostate "educational" sessions at ASTRO during the past few years. Almost all of the "experts" promoted rectal spacers while in the real world (SDN consensus) this is unnecessary.Hahahaha I know I was trying to word it in a way where it didn't force you (or anyone else) into a defensive corner because that's not my intent.
I can only speak for myself and my personal experience with it, which doesn't exactly answer my own question. I've used the goo in two very different settings. One was your standard "massive urban academic mothership". That setting forced everyone "closer to the average", meaning that there were specific things people did, or did not, do that I did or did not agree with, but nothing was so obviously good or bad that I felt like spacers were worth it.
That's actually why I started questioning this in the first place. I was in residency at a time where I watched the rise of gel, and saw the before and after. I also would rotate at a community site that didn't use the gel routinely. I just...didn't see the point, no one did any different, except one group of guys had extra needles shoved in them.
In the other setting, I had a partner who was very not good at this. The gel was the only thing between the patient's rectum and full dose, both literally and figuratively.
DON'T GET ME STARTED.
All this effort and arguments about like...millimeter PTV adjustments, no one wants to write consensus guidelines on CBCT review and whatnot??? Gah.
I've tried several things. I find having a very simple printed page to give patients explaining bowel and bladder prep helpful. Patients will do strange things about bladder filling if left to their own imagination.
In the end, asking the patients to not eat half green bananas, telling dosimetry and the therapists what I generally look for but not being a psychopath perfectionist, contouring and using PRV expansions thoughtfully - it's just a bunch of little things at each step. I like to do what I call "leapfrogging", which is having guys with gassy rectums at cone beam get off the table, go for a walk, the therapists treat the next patient, then we try again. Fixes it like...70% of the time.
I also aggressively make people use probiotics.
In the end, I rarely have GI tox. However, I can't shake GU issues. Usually urgency.
Who's got tricks for that?
I'm curious for your tips on the bolded. Most of what I've seen don't recommend any specific rectal interventions in the era of CBCTs.
You tend to have super well thought out tips, so figured I'd ask 😊
A prostate "expert" is the equivalent of a surgical "expert" in port placement. Much of their "expertise" revolves around ADT which they dont even prescribe. I know of no other analagous "expert" in medicine. Obviously they are going to be all over anything new in this space, given the absurdity of their expertise.Here's the issue. Go back and watch the prostate "educational" sessions at ASTRO during the past few years. Almost all of the "experts" promoted rectal spacers while in the real world (SDN consensus) this is unnecessary.
Worse it is yet another thing that further muddies the waters for a patient to pursue prostate radiotherapy in addition to choice of fractionation, machine brand and model, protons, MR linac, academic medical center and academic satellite treatment, robotic surgery, HIFU, active surveillance, etc. From my experience a very minor factor but still comes up.
I can't wait for the ESE, MD, PhD textbook of radiation oncology. I'll replace my old Gunderson and Tepper in a heartbeart.Oh and just to state the obvious - your Dosimetrist matters. Or Dosimetry team. Or whatever.
Part of the reason I took my current job was the Dosimetry situation seemed awesome.
And I started working here and...yeah. Best Dosimetry skills ever.
Definitely makes a difference in terms of side effects.
All this effort and arguments about like...millimeter PTV adjustments, no one wants to write consensus guidelines on CBCT review and whatnot??? Gah.
I've tried several things. I find having a very simple printed page to give patients explaining bowel and bladder prep helpful. Patients will do strange things about bladder filling if left to their own imagination.
In the end, asking the patients to not eat half green bananas, telling dosimetry and the therapists what I generally look for but not being a psychopath perfectionist, contouring and using PRV expansions thoughtfully - it's just a bunch of little things at each step. I like to do what I call "leapfrogging", which is having guys with gassy rectums at cone beam get off the table, go for a walk, the therapists treat the next patient, then we try again. Fixes it like...70% of the time.
I also aggressively make people use probiotics.
In the end, I rarely have GI tox. However, I can't shake GU issues. Usually urgency.
Who's got tricks for that?
Thanks for the detail! I'm learning some new tricks.Do you ask your prostate patients to try to have an empty rectum for CT sim and daily treatment?
I'm not a believer in daily enema or daily balloon, but just confirming that they have a BM every day before they come in (and supplementing with a laxative to titrate to daily BM prior to RT if they are not regular on their own) is an important part of my practice. I also verify that the rectum is not excessively large in the A/P diameter at CT sim - my goal is < 3cm max AP dimension, but will accept up to 4 if we've had patient walk around, try to poop, etc. In really poor performers for rectal management despite attempts to get them to walk around or even bring them back for re-sim after laxative regimen, I do increase my PTV margin from 3 to 5mm posteriorly to account for the potential emptying of rectum and posterior shifting that may not be imminently visible even on a CBCT...
I'm not a fan of enema pre-CT sim because then it's not necessarily going to be reproducible day to day.
Pun intended. If you catch that "score 3" infiltration it may very well save the patient's ass.
A prostate "expert" is the equivalent of a surgical "expert" in port placement. Much of their "expertise" revolves around ADT which they dont even prescribe. I know of no other analagous "expert" in medicine. Obviously they are going to be all over anything new in this space, given the absurdity of their expertise.
No gel is best gel.Dr. Hansen with the only data-driven take
I would like to see the COI for the guy touting balloon
Game changing paradigm shiftI would like to see the COI for the guy touting balloon
"I also was an investigator in a recently completed FDA pivotal trial for a completely novel next generation spacer which is NOT a gel, but an injectable biodegradable balloon. It is a game-changer."
Did $$ change hands?
Everyone’s bedroom choices are their own!Maybe it's just me, but I don't really want a dissolvable balloon inserted into my body.
I can't wait for the ESE, MD, PhD textbook of radiation oncology. I'll replace my old Gunderson and Tepper in a heartbeart.
Now I am dying to know what your dosimetrists do differently!
I typically talk to them about them about bladder filling in detail. "Get a water bottle, pee x amount of time prior, drink a standard amount of water before coming and don't pee until we're done" I tell them that "ideally" we'd want a bowel movement prior but I haven't typically gone to the extent of prescribing laxatives or enemas. We do give dietary guidance. Never tried probiotics -- what do you recommend for them? Definitely find we get patients off the table and walking a fair amount when things don't line up.
Thanks for the detail! I'm learning some new tricks.
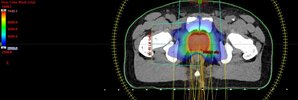
This is what every plan should look like.Our physics and dosimetry team recently rolled out a prostate rapid plan (Varian machine learning planning) for our prostate planning and the quality of plans improved significantly across the board, most noticeable in dose fall of posteriorly into the rectum. Here is a sample plan , 70 Gy/28 fx with the color wash set to 25 Gy. I have also stopped doing SpaceOAR.
I'm sorry to say, but your dosimetry team is probably lacking if they needed rapid plan to improve their plans.Our physics and dosimetry team recently rolled out a prostate rapid plan (Varian machine learning planning) for our prostate planning and the quality of plans improved significantly across the board, most noticeable in dose fall of posteriorly into the rectum. Here is a sample plan , 70 Gy/28 fx with the color wash set to 25 Gy. I have also stopped doing SpaceOAR.
the quality of plans improved significantly across the board, most noticeable in dose fall of posteriorly into the rectum.
When you have to work this hard to show a benefit, maybe you should be working on something else.