- Joined
- Sep 11, 2020
- Messages
- 79
- Reaction score
- 178
Rad Onc programs deciding to SOAP


This is true. People who end up in that situation won't speak up about it.
"Wait..... so you scored 260 on Step 1, Honored all your clinical rotations, were inducted into AOA..... and now you're unemployed?"
Not so smart are ya.....
They won't speak up because its embarrassing.
We should have a separate thread anonymously reporting these cases.... if you know of two individuals that can't find jobs it means there are many, many more out there.
Boomer vs Millennial in a nutshell - "what's good for me" vs "what's good for the group"We'll be down a spot which as caused an ego bruise with the older faculty but is seen as honorable within the younger faculty.
Conversely, if you thought the Biochemistry minutiae of Step 1 was totally warranted and thought "I wish I could answer more trivia questions like my career depended on it", RadOnc is for you!Just as a warning to potential future applicant: If you fail USMLE Part 1 several times, you're going to have a hell of a hard time passing our board gauntlet. Worth a consideration, if you eventually want to work.
I have both “3 writtens become just one written” and “no more oral boards” on my 2020s Bingo card.Just as a warning to potential future applicant: If you fail USMLE Part 1 several times, you're going to have a hell of a hard time passing our board gauntlet. Worth a consideration, if you eventually want to work.
If the pool is indeed as cited above, something will have to give.I have both “3 writtens become just one written” and “no more oral boards” on my 2020s Bingo card.
Just as a warning to potential future applicant: If you fail USMLE Part 1 several times, you're going to have a hell of a hard time passing our board gauntlet. Worth a consideration, if you eventually want to work.
anybody who looks at curren situation, so called “older” (boomer) faculty, and is just butt hurt and annoyed about being down a resident and not having someone to do scut, should maybe retire. They have had a good run and their time has passed.Boomer vs Millennial in a nutshell - "what's good for me" vs "what's good for the group"
Was thinking more of switching to matching instead of sticking with multiple choice....I have both “3 writtens become just one written” and “no more oral boards” on my 2020s Bingo card.
Finally I am woke 😁. I have no clue what happened here at U of M (assume they matched), and when I start at UH/Case in a few months I think the caliber of any hire/recruit/match is of critical importance. Residents included and will be a major focus for the coming year.Argument was BS from the get go b/c of SOAPing. I believe I made comments stating the same in that thread four years ago. I really don't understand why anyone puts any faith in our "leadership" weather its Zietman, a newly woke KO, D. Spratt, the no SOAPing in this program pledgers or anyone else. Literally the only thing that is relevant is reducing complaint and or closing programs. When they start doing that they maybe be worth listening to.
Finally I am woke 😁. I have no clue what happened here at U of M (assume they matched), and when I start at UH/Case in a few months I think the caliber of any hire/recruit/match is of critical importance. Residents included and will be a major focus for the coming year.
SOAP is a problem, but ignores the bigger picture and bigger problem. As so many of you have said, the quality of applicants/standards have simply been lowered. That has happened even at good programs. The SOAP is an easy target to blame, but there are likely another 60+ applicants with similar or even worse applications who actually matched.
It is funny to read that ppl associate good programs with those that fully match, when that is totally based on standards of who to interview and how many you interview. Standards have been massively lowered to the point I have been in shock the past few years. So much more I could say on this.
We have over expanded our field and solutions won’t come from simply PDs or Chairs or IJROBP/PRO editorials. They will come from ASTRO/ABR rules to strongly encourage = mandate Chairs/PDs follow. I had great training in NYC, but remember that MDACC, MSKCC, and HROP have ~25 slots. That means a massive percentage of our field is trained at three programs. This always blew my mind.
Programs with 1 slot each year for 4 years need to be looked at closely to why they exist. From purely an education standpoint I think 1 resident per year is too few and programs should really have 2-3 per year. Important for residents to have co residents. More than 3-4 per year I don’t see why they need more slots.
There are programs without protons, gamma knife, good brachy volume, and MR linac, etc. Ideally training programs should train residents in diverse and broad aspects of radonc.
So don’t let SOAP distract you from an increasingly saturated field that is lowering standards, and a field that needs innovation to expand RT indications.
I would have no issue with ppl filling SOAP slots if they were strong and qualified, the training program could train them in many things, and they would get a good job. Many programs are not taking strong applicants, have training programs that solely offer photon LINAC RT, and struggle for their residents to get jobs. Don’t let SOAP distract you from what is actually happening, which many of you are well aware of.
I love radonc and still believe it is an incredible field with a bright future. I am optimistic change will come, but I also understand the reality of what has and is happening and why ppl have lost hope. I am super excited to try to make change, even in a microcosm! Will work my tail off to make Case/UH a great place to train and work and not to contribute to the problem.
best
Dan, I hope when they hand you the Golden Chalice Encrusted with Diamonds filled with the Essence of the Innocent at your inaugural SCAROP meeting, that you remember these opinions.Finally I am woke 😁. I have no clue what happened here at U of M (assume they matched), and when I start at UH/Case in a few months I think the caliber of any hire/recruit/match is of critical importance. Residents included and will be a major focus for the coming year.
SOAP is a problem, but ignores the bigger picture and bigger problem. As so many of you have said, the quality of applicants/standards have simply been lowered. That has happened even at good programs. The SOAP is an easy target to blame, but there are likely another 60+ applicants with similar or even worse applications who actually matched.
It is funny to read that ppl associate good programs with those that fully match, when that is totally based on standards of who to interview and how many you interview. Standards have been massively lowered to the point I have been in shock the past few years. So much more I could say on this.
We have over expanded our field and solutions won’t come from simply PDs or Chairs or IJROBP/PRO editorials. They will come from ASTRO/ABR rules to strongly encourage = mandate Chairs/PDs follow. I had great training in NYC, but remember that MDACC, MSKCC, and HROP have ~25 slots. That means a massive percentage of our field is trained at three programs. This always blew my mind.
Programs with 1 slot each year for 4 years need to be looked at closely to why they exist. From purely an education standpoint I think 1 resident per year is too few and programs should really have 2-3 per year. Important for residents to have co residents. More than 3-4 per year I don’t see why they need more slots.
There are programs without protons, gamma knife, good brachy volume, and MR linac, etc. Ideally training programs should train residents in diverse and broad aspects of radonc.
So don’t let SOAP distract you from an increasingly saturated field that is lowering standards, and a field that needs innovation to expand RT indications.
I would have no issue with ppl filling SOAP slots if they were strong and qualified, the training program could train them in many things, and they would get a good job. Many programs are not taking strong applicants, have training programs that solely offer photon LINAC RT, and struggle for their residents to get jobs. Don’t let SOAP distract you from what is actually happening, which many of you are well aware of.
I love radonc and still believe it is an incredible field with a bright future. I am optimistic change will come, but I also understand the reality of what has and is happening and why ppl have lost hope. I am super excited to try to make change, even in a microcosm! Will work my tail off to make Case/UH a great place to train and work and not to contribute to the problem.
best
Thank you.Finally I am woke 😁. I have no clue what happened here at U of M (assume they matched), and when I start at UH/Case in a few months I think the caliber of any hire/recruit/match is of critical importance. Residents included and will be a major focus for the coming year.
SOAP is a problem, but ignores the bigger picture and bigger problem. As so many of you have said, the quality of applicants/standards have simply been lowered. That has happened even at good programs. The SOAP is an easy target to blame, but there are likely another 60+ applicants with similar or even worse applications who actually matched.
It is funny to read that ppl associate good programs with those that fully match, when that is totally based on standards of who to interview and how many you interview. Standards have been massively lowered to the point I have been in shock the past few years. So much more I could say on this.
We have over expanded our field and solutions won’t come from simply PDs or Chairs or IJROBP/PRO editorials. They will come from ASTRO/ABR rules to strongly encourage = mandate Chairs/PDs follow. I had great training in NYC, but remember that MDACC, MSKCC, and HROP have ~25 slots. That means a massive percentage of our field is trained at three programs. This always blew my mind.
Programs with 1 slot each year for 4 years need to be looked at closely to why they exist. From purely an education standpoint I think 1 resident per year is too few and programs should really have 2-3 per year. Important for residents to have co residents. More than 3-4 per year I don’t see why they need more slots.
There are programs without protons, gamma knife, good brachy volume, and MR linac, etc. Ideally training programs should train residents in diverse and broad aspects of radonc.
So don’t let SOAP distract you from an increasingly saturated field that is lowering standards, and a field that needs innovation to expand RT indications.
I would have no issue with ppl filling SOAP slots if they were strong and qualified, the training program could train them in many things, and they would get a good job. Many programs are not taking strong applicants, have training programs that solely offer photon LINAC RT, and struggle for their residents to get jobs. Don’t let SOAP distract you from what is actually happening, which many of you are well aware of.
I love radonc and still believe it is an incredible field with a bright future. I am optimistic change will come, but I also understand the reality of what has and is happening and why ppl have lost hope. I am super excited to try to make change, even in a microcosm! Will work my tail off to make Case/UH a great place to train and work and not to contribute to the problem.
best
Someones program has gotta die and the ones with the small footprint will be first...sorryHere we go with the same old "small program" blame game. That has nothing to do with it.
I came from a small program that had one of the best physics departments in the country and had all the bells and whistles in terms of tech. My education and depth of training were fantastic and I feel I am pretty competent when it comes to providing good oncology care to the community. Were there some deficiencies in my training, sure, but nothing that a prep course or working closely with some experienced providers in the modality wouldn't solve.
The problem is when I came to my last year to search for a job. Everyone ran for the hills and I was left to fend for myself. Even years later, the chair acts like he doesn't know me and like I didn't spend 4 years in his department supporting his clinical and research programs.
The reason quality applicants don't apply anymore is that they can read between the lines and see this lack of support.
They can see the board certification process becoming too burdensome of a gauntlet to traverse (ie 4 difficult tests, some of which the bar arbitrarily gets set even higher to pass).
They can see the lack of support practicing clinicians get with new reimbursement models that will make it hard for many clinics to survive, let alone all the new prior authorization companies private payers are using to deny payment and make even standard treatments hard to get approval.
They see an end of the line specialty that needs to grovel at the feet of others to support their clinics, without any real ownership of any disease site.
They see the lack of any real funding to support their research endeavors and lack of any protected time to get meaningful research done.
They see a field that is simply not worth their time.
I just hope he doesnt turn into some side show chair that SDN supports but really nobody else listens to in the rest of the world. But yeah I like himWell, I guess Cleveland now houses another rad onc with some stones to tell the truth.
I swore I wouldn’t do it, but if Spratt goes shirtless, face painted, with bull horns on head and storms the ASTRO plenary stage I will faithfully join him.
I just hope he doesnt turn into some side show chair that SDN supports but really nobody else listens to in the rest of the world. But yeah I like him
We shall see. Rarely looking to sit on the sidelines. Try to pop on here now and then as diversity of opinions valuable. Leaders who lose touch are flying blind. Plus it keeps me humble when I read ppl hating on me 😁. No one is perfect.I just hope he doesnt turn into some side show chair that SDN supports but really nobody else listens to in the rest of the world. But yeah I like him
Equipment my practice has: very good
Equipment my practice does not have: expensive, unproven, who will pay for this???
shut down all hellpits without all modalities!!!!
Grubbe-Here we go with the same old "small program" blame game. That has nothing to do with it.
I came from a small program that had one of the best physics departments in the country and had all the bells and whistles in terms of tech. My education and depth of training were fantastic and I feel I am pretty competent when it comes to providing good oncology care to the community. Were there some deficiencies in my training, sure, but nothing that a prep course or working closely with some experienced providers in the modality wouldn't solve.
The problem is when I came to my last year to search for a job. Everyone ran for the hills and I was left to fend for myself. Even years later, the chair acts like he doesn't know me and like I didn't spend 4 years in his department supporting his clinical and research programs.
The reason quality applicants don't apply anymore is that they can read between the lines and see this lack of support.
They can see the board certification process becoming too burdensome of a gauntlet to traverse (ie 4 difficult tests, some of which the bar arbitrarily gets set even higher to pass).
They can see the lack of support practicing clinicians get with new reimbursement models that will make it hard for many clinics to survive, let alone all the new prior authorization companies private payers are using to deny payment and make even standard treatments hard to get approval.
They see an end of the line specialty that needs to grovel at the feet of others to support their clinics, without any real ownership of any disease site.
They see the lack of any real funding to support their research endeavors and lack of any protected time to get meaningful research done.
They see a field that is simply not worth their time.
I agree with many of these points, but not all. In practice you are spot on that you may need nothing more than a LINAC to treat 90%+ of patients. This is different than training. One can't predict where the field is going, and training should train people in the breadth of radonc as best as possible. Some will love brachy, some protons, some SRS, some adaptive, etc. No different than surgeons learning dozens of different surgical techniques, equipment/tools, etc, and they will decide what and how they treat patients when they get a job. If they only learned to do hernia repairs they will struggle to get a job and stay relevant. Even if they are the best at hernia repairsMy 2 cents:
1- Proton: leave it the way it was in 1990s and 2000s. Highly specialized technology that is best left with a few facilities in the country. No need for every program to own a proton machine. Every time I had a pt with base-of-skull chordoma, I sent to Boston, no problems. This is what proton is for.
Proton is not for anatomic sites with big volumes (lung, breast).
The dosimetry might look better with proton but 2 important questions (let's say lung, and breast and I will NOT get into prostate debate):
1. Is outcome better (cancer-free survival)?
2. Cost to society, who is paying for these, now with RO-APM coming...
This country is going bankrupt with significant debt ~ $28 Trillions heading to $30T soon.
Also, one cannot use technology (let's say Proton) to beat biology (nasty lung cancer that is IIIB)...to quote Dr Lester J. Peters...
2- Gamma Knife: many places I know are decommissioning GF bc the majority of the depts in the US can offer SRS or SRT (with or without mask). GF had its days, it is going the way of cassette tapes and VHS tapes.
So the SRS training is basically standard in any program now. Basically treating most mets with SRS or SRT.
3- Brachy: yes some programs don't have good brachy volumes, simply bc technology such as IMRT sadly replaces good brachy.
Prostate brachy will go the wayside soon bc EBRT is as good as brachy without the anesthesia and risks involved with brachy. I have done over 1000 prostate brachy procedures in my life, I enjoyed it, but now with data from IMRT so good, why should I "torture" my patients? The last time I did prostate brachy was some 6-7 yrs ago.
The "real" brachy gurus have slowly retired (Syed, Goffinet, L. Harrison), there are few gurus remaining.
How many people really know how to do a proper oral tongue implant or a good vaginal interstitial, very few...
How many people know how to do soft tissue sarcoma brachy, very few...
4- MRI-Linac: of course on paper, it looks better. But on the long run, it will not affect the ultimate outcome, which is cure of cancer.
MRI-Linac, to me, is a just a Nintendo...Will see how long the Nitendo lasts...
The cost to society is significant, and yet there is no data to support its use.
Who is paying for this: the pt or society?
This is where the field is heading in the wrong direction: significant investment for doubtful outcome.
Again, technology cannot beat the biology.
I have to agree with RW that we need smart physician-scientists, not so much for radonc itself, but for discovery of new cancer treatments, whether it is IO or some other modalities. But my guess is that out of 100 radoncs, only 5% or so should be in the labs, the rest 95% still have to to do the "dirty job", providing safe/effective/outstanding/compassionate care for our cancer pts at as-low-as-reasonably-achieved (ALARA) cost.
We need to advance basic science bc there is where the future is...but only 5% of us need to be in the labs....
5- Program size: I have seen outstanding radonc from small programs with 1 to 1.5 residents/yr.
I have seen horrible radonc from one of the big three you mentioned above: terrible bedside manner, not up-to-date etc.
It all depends on the trainee's desire to read/learn/have discipline...
So closing a program bc it is small in size is NOT a good idea.
Why was Cornell closed, it was not a small program?
Just look back at 1990s data and scale program size back down and things will be fine.
This field has not had good leadership in the last 20 years...
") I wish I had exposure to more than just brachy and photons in training, and that was when there were very few proton centers, no MR Linacs, etc. Now it is even more important for trainees to have this exposure and experience.
I wish I had exposure to more than just brachy and photons in training, and that was when there were very few proton centers, no MR Linacs, etc. Now it is even more important for trainees to have this exposure and experience.It's been quite a party thus far with academic centers able to efficiently absorb the slack in the market by having obscene profit margins built on the back of private insurance companies. (And thus why most rad oncs working in US are now academic, or "academic.") ASTRO "lost their s**t* over APM because it saw a gravy train ending that those in the community were kind of "meh" to. A proforma for a CMS patient with MRgRT looks incredible right now; it'll look pretty scary to buy a $6+ million dollar machine if that proforma looks the same regardless the machine. If private insurance adopts APM pricing, the "arms race" era of rad onc (oh you got protons? me too! oh you got an MRgRT machine? me too!) will be on the ropes.I wish I had exposure to more than just brachy and photons in training, and that was when there were very few proton centers, no MR Linacs, etc. Now it is even more important for trainees to have this exposure and experience.
As a dosimetrist, I'm disturbed that this place is ACR accredited.
Fortunately, I've only got a few months left of training, so I can easily just reply to the email my PD will send out with "WELCOME!" or something equivalently cheesy/insignificant, and then never talk to these kids again.Will you guys/gals be happy for the students who match into your programs?
Wow... this can’t be realNow *this* is choosing violence!
Lol, definitely a fake account. Joined March 2021, 1 follower.Wow... this can’t be real
? The acr accreditation?Wow... this can’t be real
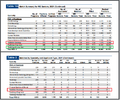
54% US MD seniors. 5.8% US DO seniors. Rest unfilled or FMG.It looks like 35 unfilled positions for programs offering PGY-2 positions. https://mk0nrmp3oyqui6wqfm.kinstacd...ds/2021/03/Advance-Data-Tables-2021_Final.pdf
I came here to say this and you nailed it. The old posts of "anonymous interview reviews" were a gold mine when getting a flavor of programs. What if we had a thread on Tales from the Job Hunt? Could be sent to @Neuronix and posted anonymously. I personally know of 3 people from this year who got quite far in the interview process only to have a job vaporize. Doesn't do much good with me reporting that, we need the firsthand accounts. @radonc17 already shared a bit about the RadOnc vs MedOnc job hunt. Would love to hear more like that. Cities and regions could be changed to protect the innocent.
The surveys are being done and there are real benefits to publishing these, but we all know the drawbacks when your preferred geographic region is inclusive of CA and Idaho. This could be the next best thing, a case series. I think getting something like this going before the intriguing April 1st Existential Threat Zoom Summit would be useful.
54% US MD seniors. 5.8% US DO seniors. Rest unfilled or FMG.
Like completely inconceivable a decade ago.