Just took the QE for the first time and passed. I found these forums to be helpful, so I wanted to chip in my experience. In short, I waited 2 years to take the QE, against the advice of many people who said “take it as soon as possible!” I chose to finish my one-year fellowship without worrying about boards and to spend another year to take my time & prepare for the QE, looks like it’s worked out so far.
The remainder of this post is fairly lengthy, in part because I felt that I could never have enough data to work from when preparing for the QE.
Textbooks: I never really believed all the people that said “read ___ cover-to-cover” - I would read a chapter for weekly lectures and forget over half the material, not even to mention the esoteric testable content. I read the Whipple chapter from Mastery at least 3 times and still only retained about 60% of it. I was advised early on that being a good surgeon and passing the ABSITE were both obligatory and distinct objectives, and there was no reason to assume that one would facilitate the other, so I wasn’t big on the cover-to-cover method.
ABSITE: I was never great at ABSITEs, started in the 9th percentile, and ranged from 20s-70s. The biggest jump for me came after taking an ABSITE course (ABSITE Review), which I subsequently took every year after that. I still was never a star, but was able to at least stay employed.
Deferring QE opportunities: one of the alumni from the fellowship I went to was the lone voice that advised me to defer the QE until after fellowship. He took it during fellowship, failed, and felt that he didn’t have enough time to prepare. Everyone else said to take it while the material was fresh from residency. I figured some of those people genuinely wanted me to pass, others just wanted to rationalize why they should get their own boards over with as soon as possible.
As a devil’s advocate, I’d say that with so much at stake, why would I want to get it over as soon as possible? If you’re a patient getting a Whipple, do you want the guy who gets it over as soon as possible or the guy who did everything reasonably conceivable to achieve meticulous resection & reconstruction? Re: what was at stake, our chairman pointed out that in legal matters, attorneys would have access to our first-time board pass rate and if sued could pursue a line of questioning of “So most surgeons pass the boards on their first attempt, did you?” Obviously the accreditation status of my residency also weighed on my conscience.
In addition, I hoped (and was found to be correct) that my first year of practice offered me more time to study than my chief year of residency or my one year of fellowship. I definitely had more freedom in time off to go to courses. Speaking of which:
QE Prep: Since I had deferred for two years, I wanted to at least prove to myself that my training regimen would exceed the average regimen. I went to three courses and did about 2000 questions twice. I really struggle to have the attention span for reading undirected primary material, so I didn’t make any effort to read anything “cover-to-cover.” My plan adapted as the year went along, but this is ultimately what I did:
-December: ABSITE Review Course
-January: ABSITE course at St. Barnabas in New Jersey
-January: Take the ABSITE
-2 x SESAP 13, 14, 15
-2 x Fiser
-A couple hundred SCORE questions
-July: Osler Course
-July: QE
ABSITE Review course: this is the ~$500 course offered at Chicago, Atlanta, LA, Vegas. I have taken this course at least 6 times in my life, It’s virtually identical every time. While there is some value, I’d say it’s among the lowest yield products out there. The printed materials are full of typos, only line up with the talks about 90% of the time, and the exact same errors persist year after year. One of the 3 speakers (Mahmoud) is a really nice guy, but not particularly gifted in oration. He was also a speaker at Osler, and was definitely in the bottom quartile of teaching ability there.
ABSITE course at St. Barnabas in New Jersey: this is the highest yield ABSITE course I’ve taken. Dr. Chamberlain puts together an excellent curriculum with excellent speakers. They explain a little more of the concepts than ABSITE Review, they’re more entertaining, the food is better, and it’s like a quarter of the price (< $200, feels like robbery). This course is not publicly advertised or Google-accessible, and I don't want to compromise their privacy if they're doing it intentionally. If you want to find a contact person, get in touch with the people that run the general surgery residency there, they should be able to get you into the right channels.
ABSITE: I hadn’t done much studying other than going to these two weekend courses, so this turned out to be more of a diagnostic test of where I stood before doing a bunch of study questions. They don’t give you a percentage as an attending, but I got 68% correct.
As a reference, over the prior 6 exams, I scored 69 - 79% correct, this was a range of 28 - 73rd percentile. So I knew that I had scored the lowest as my diagnostic score, and that it was less than 35th percentile of 3rd year residents. On the QE, I scored pretty much in the middle of the pack, and it appears that they fail about 20%.
I also want to point out that contrary to what many people told me, I felt that the QE was more similar to the ABSITE than anything else I could compare it to. Every single question I got felt like something I would or could have seen on an ABSITE. Although some questions had some complexity, I didn’t see any that reached the complexity of a typical SESAP question. Many were straightforward first-level questions. There was a mix of 4-choice answers and 5-choice answers, maybe 20% 4-choice. Several people told me it was so different that taking ABSITE review courses was a waste of time; in retrospect, I would fully disagree with that sentiment.
Fiser: Over the last 7 years, I’ve found Fiser’s ABSITE Review Questions to be more similar to ABSITE questions than anything else I’ve seen (SCORE, SESAP, Rush, Hopkins). I’ve been through my book of 580 questions at least 10 times in my life, so it only takes about an hour or two to flip through it, but I still found it useful. I did it once during the spring, marked the questions I got wrong, and then looked at the wrong questions the day before the exam.
SESAP: This forum seemed to consistently recommend SESAP, so I put some effort into getting as much SESAP exposure as possible. As some have mentioned, it is very difficult to get SESAP once a new version is released. I had SESAP 13 from residency, and SESAP 15 is the current version so I got that one too. I had my local library obtain SESAP 14 from the National Library of Medicine as an interlibrary loan (although they were only able to get the first of the two volumes). The most accurate advice I heard about SESAP was at the end of my training regimen from an Osler instructor: “I did SESAP and only got about half right..the real value is in the explanations.”
I was able to go through SESAP 13 & 15 twice through the Spring without much difficulty in time management, I was surprised when I heard from a Plastics fellow that she “did SESAP” but did not complete even a single year’s database of questions. Of note, she passed the QE on her first attempt. I got SESAP 14 later in the game and had to hustle, and found that I did in general get bogged down spending a long time trying to pick a best answer, while probably the actual value was in the explanation of the answer that I had yet to look at. I embraced the struggle to find a best answer out of 5 very lengthy answer choices because I thought this was most representative of the QE, when in fact, I found the QE noticeably less verbose and less complex.
For all three of the SESAP databases, I was getting around 30% correct on my first attempts - this was a point of some concern to me, as I all the people I talked to were scoring in the 50-60% range.
Of tangential interest, at the Osler course, there were many questions directed to the instructors that began with “..but in SESAP, it says..” That indicated to me that SESAP was a very prevalent source, and that many of our peers have synthesized the information and have it at immediate recall.
The Johns Hopkins ABSITE Review Manual is a nice collection of questions that I used during residency and had found slightly more rigorous than Fiser and more ABSITE-like than SESAP, but I didn’t end up using it because so many people had told me the QE was different than the ABSITE. In retrospect, this probably would have been time well spent.
SCORE is allegedly exactly what the QE is derived from, but I found the questions to be pretty low yield. Many questions had little or even no explanation. In addition, the primary sources from which they are derived (usually Greenfield) had minimal exposition on the content that would help me answer similar questions. On many questions, you could derive the correct answer without any content knowledge simply based on how the answers were written (something like “A) all ___ are lethal” – we all know that answers with absolute expressions are wrong), which I did not feel was representative of the QE. Since the SCORE questions felt quite different from Fiser or SESAP, I didn’t spend that much time on them. In retrospect, I’m surprised that so many people espouse its reliability.
Osler: I met a lot of haters on Osler, but I found it to be overall the most useful product I used. There was enough time (4-5 days instead of a weekend) to cover the lion’s share of the material, they did a bunch of questions, they gave good explanations, and it was helpful to observe and chat with other serious test takers. Also, if you fail, you can retake the course for free. Some of the speakers were truly superb, and gave me a better understanding of some major concepts than I had ever had throughout residency (Peds Surgery, Oncology). St. Barnabas had several content experts, but Osler had an actual ENT give the ENT talk, among other experts. I had memorized rat facts about ENT for 7 years and never understood any of them; after a one-hour lecture, I understood dramatically more - and I could ask them clarifying questions afterwards.
I took Osler a week before the exam, as it’s designed, and had my first sign of reassurance in my training regimen that I might pass the QE when the instructor went through 50 questions at the end of the first day and I got 90% correct, and fully understood the material of the 10% I missed. I had been doing SESAP questions where I was getting 30% correct, and about half the questions I got wrong, I had no grasp at all of the specific content being examined.
Some people comment on the expense of these courses. This is strange to me. Our careers are worth millions of dollars - a typical surgical specialist may pull $300k/year over a 30-year career - that’s $9M, plus benefits. Can you imagine an NBA player signing a $9M contract with the Lakers, then complaining that he had to spend $5000 on some portion of his training?
QE: I used all the simple tricks I could think of for the last week of prep. To combat jet lag to Osler and to be able to retain as much of the lecture material as I could, I took Ambien to get enough sleep and caffeine tablets to stay awake; I guess it was prophylactic since I hadn’t actually had difficulty sleeping or staying awake yet, but I knew from prior experience that I probably would. I worked out every day of the course to try to keep some metabolic activity going after sitting in lecture for 10 hours a day.
For the QE, I took the day off from work the day before, worked out, and flipped through some question bank material that I had set aside in advance to review on the day before. I tried to plan out most of the last 24 hours before the exam in advance to minimize the decision making and unpredictability immediately before the exam. I took Ambien the night before. I prepared a light lunch, low on carbs. Caffeinated at the beginning and midpoint of the exam. Brought layered clothing and comfortable shoes & pants. Kept some candy and fruit in my locker for energy boosts and something to look forward to during breaks. I made plans to do something fun at the end to have something to look forward to.
One month later, I was standing next to the scrub sink and saw old friends posting #passedboards on Facebook. I checked the ABS website with great apprehension and found that I had passed the QE. To the future examinees that read this: you are already surgeons. I wish you the best of luck and hope that you will have the same success.
Appendix:
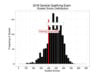
I’ve attached two pieces of data from my letter of qualification that was not available to me prior to the exam. One shows the bell curve of the examinees, with the mark that they set for passing. You can see the distribution of the scores and how they have about 20% fail each year.
The second image is an explanation where they state in broad strokes their algorithm. I don’t really understand what it means, maybe some of the readers will. It is my belief, and it annoys me that this could be true, that the ABS intentionally fails 20% of the examinees. These are actual surgeons - physicians who have been doctors for over half a decade, with hospital privileges, individuals that have spent over a decade of concerted effort and supranormal work schedules - and our national organization has a blanket policy that they should fail 20% of them. In every other professional training pathway that I’ve seen (EMT, ACLS, ATLS, ATOM), the curriculum is designed to get every willing participant to pass. Why is this one designed to get 20% of us to fail?
The second image includes a sentence that states, “theoretically, all examinees could pass (or fail) each year; there is no pre-designated failure rate on the Qualifying Exam.” I had read this prior to the exam and took false consolation in the idea that perhaps this exam was not curved, and we could all pass if we were qualified. They also state that “passing scores are determined each year through psychometric analysis and comparison with previous examinations so that the passing score is comparable from year to year. This way, examinees have the same chance of passing regardless of the examination year..or ability of the overall examinee group.” Taken together, one could surmise that there is no curve.
On the other hand, I also know:
1. the percentage of passing examinees has a range of only 2% over the last 5 years (79% - 81%),
2. the threshold for passing is determined after the test is administered, and is chosen to retain consistency (as described above)
I’m not a statistical expert, but these two facts together describe to me a curve with a pre-determined fail rate. It could be true that you are not specifically competing against the other examinees in your year, but for all meaningful intents and purposes, you have to be better than 20% of your peers to pass.