D
deleted941485
I mean Seriosuly what else does RO have going for it?

I thought Nancy lee was implicitly criticizing protons, saying they have become too big too fail.Nancy Lee has the higher ground
Bubbles all around us.Proton cash is absolutely keeping the job market alive.
It’s sick
EVERYTHING. Now, more than ever.I mean Seriosuly what else does RO have going for it?
Not what i got from her statementsI thought Nancy lee was implicitly criticizing protons, saying they have become too big too fail.
Wide scale adoption of protons will HAVE to lead to a steep price correction like IMRT, right??? Right???


And owning a piece i guessfrom a source - I am now hearing that UHC is uniformly approving proton for prostate cancer, no fights needed. Proton lobby wins again. This must be a downstream effect of big lawsuits.
from a source - I am now hearing that UHC is uniformly approving proton for prostate cancer, no fights needed. Proton lobby wins again. This must be a downstream effect of big lawsuits.
This is one of those pieces of info that if rad oncs and all academicians truly understood/came to grips with, we would all be so much better offIn a lot of these cases, uhc is just acting as a fiducial/middle man for the employer. (Unless Medicare advantage) Higher billing is better for their bottom line.
It’s a very ugly synergy between hospitals and payors at the heart of health care price dysfunction.This is one of those pieces of info that if rad oncs and all academicians truly understood/came to grips with, we would all be so much better off
And ASTRO wants to gripe about urologists buying linacs and overutilizing (I thought RT is a valid tx option for any and every localized prostate cancer patient?) radiation therapy. I never had anything to do with a urorads type place nor knew anyone who worked there. But this was ASTRO attacking its own members who had chosen to go work in these settings. That’s when I had to drop my ASTRO membership because I knew that maybe one day I might be a member whose practice and employment they looked down on. Their open animosity got too vociferous.It’s a very ugly synergy between hospitals and payors at the heart of health care price dysfunction.
...and don't get me started on pineapple ripeness.And ASTRO wants to gripe about urologists buying linacs and overutilizing (I thought RT is a valid tx option for any and every localized prostate cancer patient?) radiation therapy. I never had anything to do with a urorads type place nor knew anyone who worked there. But this was ASTRO attacking its own members who had chosen to go work in these settings. That’s when I had to drop my ASTRO membership because I knew that maybe one day I might be a member whose practice and employment they looked down on. Their open animosity got too vociferous.
You're not paranoid, it's true.
United Healthcare is trying to make money from protons. It is listed by the SEC as owning "ProHealth Proton Center Management, LLC" and is one of the major investors of the NYPC, along with Mount Sinai, MSKCC, and Montefiore:
New York State’s first Proton Therapy Center reaches completion
www.stantec.com
"New York Proton Management, LLC" is another subsidiary on this SEC document regarding UnitedHealthcare.
Document
www.sec.gov
I think this could be construed as a conflict of interest pretty easily.
The suite you link to was filed in 2019United Healthcare.
Wonder what is happening with this?

When insurance companies came up with the phrase "Experimental and/or Investigational" to deny care for things like proton beam therapy (wholly on a different level versus snake oil, laetrile, etc)... or IMRT for whole breast etc etc... it was one of the greatest verbal legerdemains ever pulled.United Healthcare.
Wonder what is happening with this?
When insurance companies came up with the phrase "Experimental and/or Investigational" to deny care for things like proton beam therapy (wholly on a different level versus snake oil, laetrile, etc)... or IMRT for whole breast etc etc... it was one of the greatest verbal legerdemains ever pulled.
It's like calling someone a racist or a Nazi in a debate. It shuts down all discussion. "Experimental" is a scary word. "They're doing experiments on me?!" It gives a veil of authority to the insurance company: "We know science, and this treatment is not scientific."
It's a minor turn of phrase. No one ever even thinks about it most likely. But it is quite effective.
This is the case with some insurers' contracts with some proton centers. As has been mentioned on this forum, the IMRT rate for those centers can still be excessive, and the negotiated rates would not apply to insurers (particularly if out of network) that don't have contracts with those centersMy monkey brain just sees it as so simple.
I don't understand why the insurance statement isn't:
"To this point we see no compelling data that proton therapy for prostate cancer presents any benefit or detriment over that of IMRT. We therefore agree to pay for proton therapy at previously negotiated IMRT rates until new research shows otherwise."
Penn and Mayo love to publicize that they take imrt rates for protons without mentioning these imrt rates are 5-10 x cmsThis is the case with some insurers' contracts with some proton centers. As has been mentioned on this forum, the IMRT rate for those centers can still be excessive, and the negotiated rates would not apply to insurers (particularly if out of network) that don't have contracts with those centers
At a 36 month follow up I will put a drop of Tc-99m colloid on the nipple up against proton partial breast any day.Need to do that technetium 99 localization / definitive radiotherapy noninferiority trial. I hear @TheWallnerus wants to start accrual asap.
Tell me you had to create a comparison plan for authorization without telling me you had to create a comparison plan for authorization.
DING DING DING DING!!!Tell me you had to create a comparison plan for authorization without telling me you had to create a comparison plan for authorization.
It's this kind of equipoise and academic honesty you can expect in rad onc these days.DING DING DING DING!!!
Tell me you had to create a comparison plan for authorization without telling me you had to create a comparison plan for authorization.
It’s hard to read a rad onc article in a journal these days without it making me mad; the type of anger you feel when someone tries to play you for a foolThey should have been embarrassed to publish that "comparison" - I'd love to see an IMRT partial breast plan compared to their ridiculous proton grift.
Red urinal isn't worth the TP it's printed on. Stick to JCO nejm jama lancet imoIt’s hard to read a rad onc article in a journal these days without it making me mad; the type of anger you feel when someone tries to play you for a fool
Man RJ is so dismal nowRed urinal isn't worth the TP it's printed on. Stick to JCO nejm jama lancet imo
Mirrors the health of our specialtyMan RJ is so dismal now
So many of our seminal papers were from there in the past.
And now…
Mirrors the health of our specialty
Hey now!Saw they put out a whole review on LDRT for OA. I read every page of it and came away thinking gosh what the hell did I just put myself through.
Would say they could offer us semenal papers now, but we are out of the testicular cancer game too so not even thatMan RJ is so dismal now
So many of our seminal papers were from there in the past.
And now…
StretchWould say they could offer us semenal papers now, but we are out of the testicular cancer game too so not even that
I’m going to also go on a rant on #5What's frustrating is that there is indeed low-hanging fruit that should be investigated IN PHASE III CLINICAL TRIALS:
1. neoadjuvant Chemoimmunotherapy followed by surgery vs chemoimmunotherapy + RT + immunotherapy for IIIA NSCLC
2. Dose escalation for NSCLC with IMRT required
3. Dose de-escalation for HPV+ H+N ca, but done in a way which makes sense (60 or 66 Gy vs 70 Gy with platinum perhaps?)
4. Chemoembolization vs SBRT vs RFA vs microwave ablation for liver mets
5. Appropriate dosing strategies in skin cancer (seriously it's the wild west out there)
6. Dose escalation to 50 Gy in 5 fx with SBRT for high-risk prostate cancer with SpaceOAR required
7. SBRT for oligomets - I know we have COMET II coming out, but we should have multiple institutions investigating multiple strategies to help determine when we can derive the most benefit from treating oligomets. That's not what I'm seeing.
I'm no academician, and these are off the top of my head. So, there are probably some issues with them, and maybe there are trials in the works. We shall see.
Great post!I’m going to also go on a rant on #5
I treat a lot of skin. A LOT. Orthovoltage, electrons, VMAT, you name it. Converting some of my breast consult space for even more skin space between my RO skin partner and I.
The wild west is probably a good way of putting it. I spent a lot of my time early on in my (still junior) practice on reviewing strategies here. I could go on a rant here for about an hour on how no one can agree on how to treat this.
I‘ll attach a few dose and fractionations that come from different sources. Note whiel there are some commonalities, in other cases they are WILDLY different.
ASTRO guidelines:
View attachment 359637
NCCN:
View attachment 359638
Some US dermatology guidelines:
View attachment 359639
This one I think is hilarious because it references ‘Total Dose Fractions’ and puts the units in Gy instead of its proper/original nomenclature.
Taken from the old Orton and Ellis tables courtesy this book:
View attachment 359647
View attachment 359640
View attachment 359641
From a UK patterns of practice survey, McPartlin BJR 2014
View attachment 359642
View attachment 359643
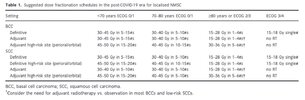
One opinion paper post covid suggests rather hypofrac/descalation of treatment for a lot of these frail patients:
View attachment 359645
Let alone some of the more recent skin SBRT publications looking at dose escalated treatment for more bulky skin cancers.
Heck, someone I used to train with used what is usually published as a HDR brachy dose with good effect, also not in any of these above. ‘The secret sauce’
One thing I’ve tried to come to terms with is what is an effective tumorcidal dose? It’s nice to try and say to give a 85 yr old 30 fractions but it’s really not practical and there are other good hypofractionation options that may be more suitable.
Also what’s hard with this - a lot of these institutional outcomes don’t report technique well. Few places have access to superficial radiotherapy, electrons are a lot more common in places that have linacs. Are these corrected for RBE, do they even need to be corrected to RBE? Are they being prescribed to 90%, is this being prescribed to Dmax? A lot of these details are not reported, and I think it matters.
What I will say which (somewhat) perplexes me and have given some thought to, is a lot of these doses if you look at more of the moderate/extreme hypofraction (eg 5-10 fr), the linear quadratic model starts to break down for what is tumorcidal for non-bulky tumors, as compared to conventional 2Gy/fr. There does seem to be a time element that is not well captured there. There may be something to using the tdf tables, for which most/all of these doses do fall along in the ‘sweet spot’ for. Probably because they are derived from this, and not vice versa. Is there difference in LC between a tumorcidal 5 fr/7 fr/10fr/20 fr/30fr regimen? Maybe? We can’t well tease it out from our current data I think.
The Zaorsky meta-analysis is good, but without good randomized data, I don’t know if one can’t really say I think since treatments can differ in technique by quite a bit.
What to do for definitive melanoma? What is effective palliation for melanoma/SCC on IO - is daily treatment truly the best?
This stuff drives me nuts. I wish we had better trials and data past - “we did this and it worked”
Also - if anyone has thoughts on above, would LOVE their insight & experience. I’m all ears.
Thanks!Great post!
Posted on twitter. It’s epic.Thanks!
I’m flattered. I’ll be curious to see if there is any thoughts from the broader bird audience. I would say from following a few of my predecessors patients as well as my own now, I’m starting to get a sense of what some of these be ‘hot’ and some of these ‘cool’ but not enough relapses for formal analysis sadly. Lot of reasons why people can relapse with appropriate prescriptions - not enough depth, treatment interruptions, marginal miss with tumor/inadequate margins, and just bad luck. Lot of good reasons to cool a prescription too. Thanks for sharing itPosted on twitter. It’s epic.
")