- Joined
- Nov 2, 2019
- Messages
- 3,497
- Reaction score
- 14,519

Damn! Foot in mouth!Oh my God, from the Potters editorial:
View attachment 332260
"RadOnc used to be too competitive for women and minorities" - Louis Potters, MD, FASTRO, FACR
There's no level of applause that would be too great for Shah and Royce on this one! Nice job fellas.This figure though 😢😢😢😳😳😳🤯🤯🤯
Two GREAT articles and one tone-deafeningly turdacious article. LOUIS... "Unpredictable year-to-year variability for a specialty in the United States of just over 4500 physicians is inevitable"... what if it's 5500 physicians? Because it is. And the number is (guess what) going up. 4500 is fantasy-land.
Can anyone attach the whole articles for those of us who refuse to be ASTRO members? Unbelievable that Dr. Louis Potters is able to say, apparently seriously, "all will be fine", let's keep SOAPing, by all means don't make me dictate my own notes, etc.
The Shah and Royce article is FIRE.There's no level of applause that would be too great for Shah and Royce on this one! Nice job fellas.
The Shah and Royce article is FIRE.
Really, tremendous work guys.
Could you post it?I wonder if LOUIS would be willing to give up his 1.7 million job to a minority in a dead end job who will never make even a quarter of that. Wouldnt that be something folks?! Instead he wants minority cheap labour then ship them off to a dead end job in middle of nowhere. This guy is very WOKE
A coincidence, I'm sure.agreed. Truly excellent
I’m little upset these came out AFTER med student rank lists finalized
This could have had a major impact
A coincidence, I'm sure.
Exactly, it is not like his extreme salary is justified by a body of academic work.Louis Potters writing yet another rambling stream of consciousness editorial. At the end of the day I think he is just trying to lay the ground work for the justification of the continued existence of his program. Sounds like application plummeted to his particular program this year.
"The sharp decline in the number of applicants this year needs analysis. Medical students, through discussion and on social media, are sensing that ours is not a specialty to enter if they wish to have a job at the end of their training. The talk is of an oversupply of radiation oncologists through an expansion of residency programs while changes in use of radiation oncology treatments and hypofractionation have suppressed demand. But is it that simple? We know that RO graduates are still obtaining jobs, that the population is still aging, and that new indications for radiation are arising. There remains room for us to flex our inner “therapeutic radiologist” and broaden our scope of practice beyond external beam radiation therapy into brachytherapy and radionuclide therapy. The influence of COVID-19 is also uncertain. Will physicians retire later because of income lost, or will they retire earlier because of concerns about exposure and work–life balance? To me, it does not seem clear that we are oversubscribed as a specialty.
The final year of training in any specialty, not knowing where one will live and practice, is one of the most stressful times in a young physician’s life. When there is high uncertainty, there is high anxiety. Unpredictable year-to-year variability for a specialty in the United States of just over 4500 physicians is inevitable. That was the case 30 years ago, as it is now. The remedy to manage this stress is more mentorship from attendings, program directors, and chairs working with our graduating residents to help them develop a strategy for success. In the meantime, we can take some pride in knowing that our residents are achieving their desired goals up to 82% of the time in a first job. That is a darn good batting average for such a small specialty."
This is some serious gaslightingLouis Potters writing yet another rambling stream of consciousness editorial. At the end of the day I think he is just trying to lay the ground work for the justification of the continued existence of his program. Sounds like application plummeted to his particular program this year.
"The sharp decline in the number of applicants this year needs analysis. Medical students, through discussion and on social media, are sensing that ours is not a specialty to enter if they wish to have a job at the end of their training. The talk is of an oversupply of radiation oncologists through an expansion of residency programs while changes in use of radiation oncology treatments and hypofractionation have suppressed demand. But is it that simple? We know that RO graduates are still obtaining jobs, that the population is still aging, and that new indications for radiation are arising. There remains room for us to flex our inner “therapeutic radiologist” and broaden our scope of practice beyond external beam radiation therapy into brachytherapy and radionuclide therapy. The influence of COVID-19 is also uncertain. Will physicians retire later because of income lost, or will they retire earlier because of concerns about exposure and work–life balance? To me, it does not seem clear that we are oversubscribed as a specialty.
The final year of training in any specialty, not knowing where one will live and practice, is one of the most stressful times in a young physician’s life. When there is high uncertainty, there is high anxiety. Unpredictable year-to-year variability for a specialty in the United States of just over 4500 physicians is inevitable. That was the case 30 years ago, as it is now. The remedy to manage this stress is more mentorship from attendings, program directors, and chairs working with our graduating residents to help them develop a strategy for success. In the meantime, we can take some pride in knowing that our residents are achieving their desired goals up to 82% of the time in a first job. That is a darn good batting average for such a small specialty."

Is there a reference for that? Someone once told me that new grads leave their first job within 3 years about 50% of the time (also no reference).The final year of training in any specialty, not knowing where one will live and practice, is one of the most stressful times in a young physician’s life. When there is high uncertainty, there is high anxiety. Unpredictable year-to-year variability for a specialty in the United States of just over 4500 physicians is inevitable. That was the case 30 years ago, as it is now. The remedy to manage this stress is more mentorship from attendings, program directors, and chairs working with our graduating residents to help them develop a strategy for success. In the meantime, we can take some pride in knowing that our residents are achieving their desired goals up to 82% of the time in a first job. That is a darn good batting average for such a small specialty."
Is there a reference for that? Someone once told me that new grads leave their first job within 3 years about 50% of the time (also no reference).
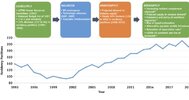
One critical distinction is the current state versus the future perception of the job market. The evidence indicates that the current state is more favorable than that of the future perception, with 82% of graduates finding a desirable job.10,24-27 Conversely, the future perception of the job market is clearly contrary, where applicants are voting with their feet and avoiding RO at historic levels.28 One point of contention that might contribute to this disconnect is this: When are job market satisfaction rates considered acceptable versus unacceptable? The trainee perspective desires job satisfaction figures as high as possible; growing education and trainee and debt A general timeline of the perceived balance of supply and demand among the radiation oncology workforce from 1993 to 2020. 2 Shah and Royce International Journal of Radiation Oncology Biology Physics burden further raise the stakes.29 A growing supplyedemand imbalance since the 2016 oversupply projections could further worsen perceptions, given the 5- year supply lag with matched and matriculated trainees in the pipeline. Conversely, other stakeholders might have lower acceptable job satisfaction rate thresholds, such as academic medical centers or entrenched professional groups that are incentivized to increase training slots irrespective of societal need.14
Is there a reference for that? Someone once told me that new grads leave their first job within 3 years about 50% of the time (also no reference).
I think that is indeed the one. It was like 82% were satisfied with at least one of three element of their job.It's probably some survey where residents said they were satisfied with EITHER job, location, pay, etc
We're also at the point where "satisfied with job" on surveys means diddly squat because residents are now satisfied with A JOB.
I agree. It is like saying I'm satisfied with being alive with food, water, and clean underwear. Remember kids, just because you love the job, doesn't mean the job loves you back.It's probably some survey where residents said they were satisfied with EITHER job, location, pay, etc
We're also at the point where "satisfied with job" on surveys means diddly squat because residents are now satisfied with A JOB.
The bright side is there is at least concensus that bad programs who cannot meet true tightening (not watered down BS) residency requirements in faculty:resident ratios, didactics, increased site requirements should be shut down ASAP. This needs to happen yesterday. Refer to worst residency experience thread aka hellpit thread.
Also he decreased his resident compliment. I got no problem with attacking his other nonsense but this is a major concession from a chair (tightening requirements and seeing where chips fall and decreasing his own program)
Wouldn’t supplementing other programs be bad for residents in top programs? I would think it would be better for top programs to be like “🤗 sucks to suck” so their grads can get the best jobs.Paradoxically, the work that is being done to ensure “educational uniformity” will ruin the chances to shut down poor performing programs
Supplementing is good in theory but it also allows poor performers to slide by since someone else is doing their job
Will be up to SIGNIF raising case minimums and having bad ACGME reviews to fix issue now
The bright side is there is at least concensus that bad programs who cannot meet true tightening (not watered down BS) residency requirements in faculty:resident ratios, didactics, increased site requirements should be shut down ASAP. This needs to happen yesterday. Refer to worst residency experience thread aka hellpit thread.
Also he decreased his resident compliment. I got no problem with attacking his other nonsense but this is a major concession from a chair (tightening requirements and seeing where chips fall and decreasing his own program)
Wouldn’t supplementing other programs be bad for residents in top programs? I would think it would be better for top programs to be like “🤗 sucks to suck” so their grads can get the best jobs.
Has potters ever had a black resident or faculty member?No programs except for those that have closed and the University of Louisville has officially decreased complement. In Potters case his, program has 8 positions and typically takes 2 residents per year. This year he will officially offer only one via the match. That other spot that was not offered in the match can be filled at anytime in the future by taking 3 next year or offering it outside of the match. That spot isn't gone until the ACGME says the program is certified for 7 positions.
If this is the standard then most “leaders” are guilty as well. You can count some of these racial minorities with your hand in our field.Has potters ever had a black resident or faculty member?
It should absolutely be the standard for anyone who tries to justify increasing trainee numbers by appealing to "diversity." Couldnt he have hired just one as a token/fig leaf over past 15 years (because he cares so much)?If this is the standard then most “leaders” are guilty as well. You can count some of these racial minorities with your hand in our field.
Look at rosters of most residency programs and their alumni. you know the answer. Howard used to have a program and it closed. Where was ASTRO when a HBC program is collapsing?Has potters ever had a black resident or faculty member?
Did Potters evolve- yes, he doesnt care about lucrative salaries unlike the gold digging residents who flocked to xrt in the golden years. He gets nearly 2 million a year (cost of living adjustment since 2018 when 1.7 million) for the right reasons.Look at rosters of most residency programs and their alumni. you know the answer. Howard used to have a program and it closed. it is simply a fact that there are few of them in our field.
it is also totally totally predatory to all of a sudden be ok with minorities. Where were these people at the peak of competitiveness and reimbursement? Sure would have been great for these minorities!!! You know to go to a fantastic program and get an amazing job!!!
the sad thing to me is these PDs did not do this when they could. Did they evolve?
I was all ready to show up to south beach.... Maybe next timeAfter reading the Shah/Royce article and the Louis Potters rebuttal, one thing is very clear...despite being presented with cold hard data, with a total of 37 citations in the Shah/Royce, all Louis Potters rebutted with is conjecture, without any substantial data and a single citation, the Shah/Royce article that he was rebutting.
To Chirag and Trevor (and many other prominent champions of our field like Simul), I will buy you a drink at the next in-person ASTRO annual meeting...if I ever decide to be a member again and go to it again.
100% truth. (Had to Google "Say's Law.")Potters is right about a couple things. Excess competition/meritocracy does decrease opportunity. It does this for everyone, not just URM or women doctors. Conflating meritocracy here with a barrier to diversity is absurd and stupid. Those URM and women applicants from 5-10 years ago were all slaying it. I personally witnessed a rank list meeting during peak radonc where multiple excellent URM applicants were given zero additional consideration in the ranking process. To be fair, gender parity was somewhat of a priority at that meeting.
IMRT coding and total compensation as a market force with negative consequences? Of course, he is right on this. But large academic institutions often cause the greatest financial toxicity. For the small minority of academic radoncs who get to run a lab, they can still bill significantly on low volume, low acuity patients (due to IMRT or heaven forbid Protons). This has been a blessing and is one of the reasons why we attracted among the best research oriented candidates during the golden era. There are not too many specialties where you take home 300K minimum while doing mostly research. There are also not too many clinical academic positions where you can take home clinical academic radonc cash (not typically 1.7M wtf) without working very long hours in the hospital.
These jobs were the fantasy of many applicants during the golden era. I met more young residency applicants ideally positioned for high powered academic and physician-scientist jobs in a single year at a single institution than such jobs were available nationally. Most of these applicants had to ultimately make significant sacrifices with job choice (location, type of practice). It's not that they are unemployed, it's that they feel underemployed and when they look at their colleagues in other fields, many view the opportunity cost as having been too high. They definitely feel underemployed compared to their predecessors from a generation earlier, who could publish a small volume in residency, demonstrate clinical acumen and have good academic opportunities (not some of these satellite jobs) or very lucrative private practice opportunities in desirable locations.
The residency expansion was just Say's law roughly. The supply of star med students (contributed to by IMRT) created a demand for star med students and has resulted in a clear oversupply. The market adjusted, the supply is gone because radonc no longer provides what a star med student wants and the programs should contract (all of them).
I personally believe that there are already more than enough clinical researchers and MD/PhDs in the field. It was magical thinking to believe highly qualified people would radically change the field. They need the intellectual space to make a big difference. We could throw the best energy researchers into coal research and they would publish and find out some stuff. They would also serve us and themselves better if they could explore alternative energy sources. Almost all the great radonc basic science researchers I know could easily be in a different department.
Would think that Ralphy (other than senility) would get this. Cant understand why any md/phd would choose radonc?Almost all the great radonc basic science researchers I know could easily be in a different department.
Graduating residents need to WISE UP when they take these surveys. The surveys are NOT benign!! The surveys are published in IJROBP and then cited by these old fogey chairs to justify the status quo of 200 residency positions per year. Every “satisfied” customer on these surveys is, consciously or not, sabotaging residency contraction and the potential redemption of the radiation oncology job market.They won't be satisfied until >50% of graduating Radiation Oncologists cannot secure jobs.
Certainly there was no discussion 10 years ago about doubling resident numbers when everyone knew hypofract was on the horizon. That did not require a range of perspectives...Graduating residents need to WISE UP when they take these surveys. The surveys are NOT benign!! The surveys are published in IJROBP and then cited by these old fogey chairs to justify the status quo of 200 residency positions per year. Every “satisfied” customer on these surveys is, consciously or not, sabotaging residency contraction and the potential redemption of the radiation oncology job market.
When Harari ain’t busy matching his son, he writes these articles.Here's another article from today from Paul Harari and crew: https://www.redjournal.org/article/S0360-3016(21)00216-9/abstract
View attachment 332306