- Joined
- Oct 17, 2011
- Messages
- 2,762
- Reaction score
- 6,278
Right now over in the ABPM/ABFAS thread we have a battle rolling over the merits of ABFAS. Whatever the merits of ABFAS may be - a review of limited historic certification data suggests that only a small cohort of each class will RRA certify (Foot is slightly more favorable)
The argument I'm going to make here has nothing to do with job opportunities, "fair", "predatory", etc. It is - it is simply a commentary on historic certification rates.
The question in my mind that lead to this thread is - what would happen if the only people who took ABFAS were the same people who succeeded in ultimately certifying ABFAS. ie. a 100% certification rate through "perfect selection" with no failed candidates dropping off along the way, wasting their time/money, becoming frustrated etc.
I am only presenting ABFAS data.
 www.abfas.org
www.abfas.org
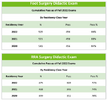
*First small thing - what are the odds that 456 people passed Foot 3 years in a row? I am open to that being a typo.
Didactic Image Here:
First off all - our data is somewhat limited. I'm not going to reach for data beyond ABFAS. I will perform a limited comparison based simply on trends of certain years while lacking other years. Above didactic data. What conclusions can be drawn from the data:
#1 - The first thing is there is a degree of self selection between people taking Foot and people taking RRA. These are the same class years so presumably these are in general the same people. It appears that approximately 90% of the people who take Foot also take RRA.
#2 - The second thing is that obviously the pass rate for RRA is substantially lower than the pass rate for Foot.
#3 - The third thing is - I don't know the graduating/matriculation rates for these years, but looking at the Foot applicant rate - I see greater than 500 students for each class taking the Foot certification test. My memory of reviewing AACPM data is that some years matriculated 600+ students. While I don't have exact data my big take home is that probably most residency graduates are ultimately pursuing ABFAS in some form or another ie. people want to be certified. Now perhaps the new ITE process means everyone tries figuring they might as well but for all the anecdotal talk of people not wanting to do surgery - a lot of people are pursuing surgical certification.
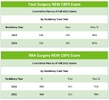
CBPS image here:
The CBPS data doesn't relay anything substantially new - the cohort size seems in line with the didactic sizes above (in general).
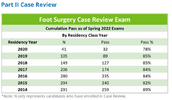
Foot Case Review Image:
#1 - Presumably (?) - individuals who pass the case review will likely certify though you can technically sit for case review by passing Part 1, but failing all portions of part 2. Obviously that would be tragic. I am somewhat viewing passing case review as a proxy for certification.
#2 - The general trend from the data suggests most people who sit for case review ultimately pass.
#3 - If you look at the residency years cohorts - the values you see for certain years are "done" ie. if you only have 7 years then no further people can sit from 2014-2016. Those values will not change. 2020 Graduates meanwhile will continue to acquire cases so the values in both N and Pass will continue to increase.
#4 - I obviously do not have data here for the number of people from earlier years who sat for didactic. However, if the values for historic didactic ie. 500ish grads, are similar to current didactic then even though the "case review pass rates" are about 80ish% - the number of people ultimately certifying in foot would be substantially beneath the number of people who started the process. For 2014-2016 - if 500ish graduates took didactic for foot then the ultimate proxiy pass rate through case review would be ~50%. Again, I don't know what number the didactic started with but there's a big drop off.
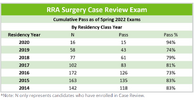
RRA Case Review Image:
#1 - Some of the same sorts of conclusions from above can likely be applied here. Theoretically case review is a proxy for certification. However, pass rates are lower compared to the rates for those who sat for Foot. Again, certain years are "done" and will have no further graduates. And again - more recent years are still acquiring cases.
#2 - I don't have data for the number of people who sat for didactics for most of these years, I acknowledge that above. If the numbers for historic years are comparable to the numbers for current years (ie. 500ish people started the process) then using RRA case review as a proxy will show a overall certification rate of less than 30%. Obviously there's a lot of assumption/extrapolation there.
#3 - On a small amusing note - my "anecdotal" feeling was that almost none of my classmates are RRA certified even though we are now several years out. In fact, there are fewer than a "podiatry school" of RRA students from my residency years.
ANYWAY. That's my rough data look. Perhaps someone with actual data can actually refute.
Let's go back to the thread title. "Reviewing historic ABFAS cert pass rates suggests you will not be RRA certified" (had to shorten to post). I chose not to touch foot in the title. I think the statistics through time are painful and I don't think the thread title is unreasonable based on what I had to work with.
Reading people's feelings on both sides of the ABFAS spectrum - its fascinating.
-If you believe ABFAS RRA helped you get a job - the simple truth is having it makes you part of a very small cohort.
-If you believe ABFAS is a scam - its hard from looking at the data not to see a massive subsidy being performed through paid testing that ultimately won't lead to certification. Essentially almost an entire class size/cohort is taking ABFAS's didactic testing but in the end only 30-50% of the class is becoming certified. There are hundreds of people per year comitting to some form of Foot/RRA testing to the tune of again hundreds of dollars who will have nothing to show for it.
-I wonder if I somehow had the current graduating class in front of me and I could poll them and ask "who here thinks they will be certified" - what would they say? How would they feel potentially seeing this historic data.
-Last of all, my suspicion is that some people would view this data as supporting the idea that the current residency RRA system is broken ie. so many 3 years graduates many with trivial RRA experience. That in fact we should go back to Foot and RRA to allow the RRA to be pooled to a smaller cohort.
Thanks for reading.
I may continue to correct small typoes after posting this. Unfortunately I could not post this with the images within the document.
The argument I'm going to make here has nothing to do with job opportunities, "fair", "predatory", etc. It is - it is simply a commentary on historic certification rates.
The question in my mind that lead to this thread is - what would happen if the only people who took ABFAS were the same people who succeeded in ultimately certifying ABFAS. ie. a 100% certification rate through "perfect selection" with no failed candidates dropping off along the way, wasting their time/money, becoming frustrated etc.
I am only presenting ABFAS data.
Exam Pass Rates
Examination pass rate data from candidates undertaking the two-step process to earn ABFAS Board Certification
www.abfas.org
*First small thing - what are the odds that 456 people passed Foot 3 years in a row? I am open to that being a typo.
Didactic Image Here:
First off all - our data is somewhat limited. I'm not going to reach for data beyond ABFAS. I will perform a limited comparison based simply on trends of certain years while lacking other years. Above didactic data. What conclusions can be drawn from the data:
#1 - The first thing is there is a degree of self selection between people taking Foot and people taking RRA. These are the same class years so presumably these are in general the same people. It appears that approximately 90% of the people who take Foot also take RRA.
#2 - The second thing is that obviously the pass rate for RRA is substantially lower than the pass rate for Foot.
#3 - The third thing is - I don't know the graduating/matriculation rates for these years, but looking at the Foot applicant rate - I see greater than 500 students for each class taking the Foot certification test. My memory of reviewing AACPM data is that some years matriculated 600+ students. While I don't have exact data my big take home is that probably most residency graduates are ultimately pursuing ABFAS in some form or another ie. people want to be certified. Now perhaps the new ITE process means everyone tries figuring they might as well but for all the anecdotal talk of people not wanting to do surgery - a lot of people are pursuing surgical certification.
CBPS image here:
The CBPS data doesn't relay anything substantially new - the cohort size seems in line with the didactic sizes above (in general).
Foot Case Review Image:
#1 - Presumably (?) - individuals who pass the case review will likely certify though you can technically sit for case review by passing Part 1, but failing all portions of part 2. Obviously that would be tragic. I am somewhat viewing passing case review as a proxy for certification.
#2 - The general trend from the data suggests most people who sit for case review ultimately pass.
#3 - If you look at the residency years cohorts - the values you see for certain years are "done" ie. if you only have 7 years then no further people can sit from 2014-2016. Those values will not change. 2020 Graduates meanwhile will continue to acquire cases so the values in both N and Pass will continue to increase.
#4 - I obviously do not have data here for the number of people from earlier years who sat for didactic. However, if the values for historic didactic ie. 500ish grads, are similar to current didactic then even though the "case review pass rates" are about 80ish% - the number of people ultimately certifying in foot would be substantially beneath the number of people who started the process. For 2014-2016 - if 500ish graduates took didactic for foot then the ultimate proxiy pass rate through case review would be ~50%. Again, I don't know what number the didactic started with but there's a big drop off.
RRA Case Review Image:
#1 - Some of the same sorts of conclusions from above can likely be applied here. Theoretically case review is a proxy for certification. However, pass rates are lower compared to the rates for those who sat for Foot. Again, certain years are "done" and will have no further graduates. And again - more recent years are still acquiring cases.
#2 - I don't have data for the number of people who sat for didactics for most of these years, I acknowledge that above. If the numbers for historic years are comparable to the numbers for current years (ie. 500ish people started the process) then using RRA case review as a proxy will show a overall certification rate of less than 30%. Obviously there's a lot of assumption/extrapolation there.
#3 - On a small amusing note - my "anecdotal" feeling was that almost none of my classmates are RRA certified even though we are now several years out. In fact, there are fewer than a "podiatry school" of RRA students from my residency years.
ANYWAY. That's my rough data look. Perhaps someone with actual data can actually refute.
Let's go back to the thread title. "Reviewing historic ABFAS cert pass rates suggests you will not be RRA certified" (had to shorten to post). I chose not to touch foot in the title. I think the statistics through time are painful and I don't think the thread title is unreasonable based on what I had to work with.
Reading people's feelings on both sides of the ABFAS spectrum - its fascinating.
-If you believe ABFAS RRA helped you get a job - the simple truth is having it makes you part of a very small cohort.
-If you believe ABFAS is a scam - its hard from looking at the data not to see a massive subsidy being performed through paid testing that ultimately won't lead to certification. Essentially almost an entire class size/cohort is taking ABFAS's didactic testing but in the end only 30-50% of the class is becoming certified. There are hundreds of people per year comitting to some form of Foot/RRA testing to the tune of again hundreds of dollars who will have nothing to show for it.
-I wonder if I somehow had the current graduating class in front of me and I could poll them and ask "who here thinks they will be certified" - what would they say? How would they feel potentially seeing this historic data.
-Last of all, my suspicion is that some people would view this data as supporting the idea that the current residency RRA system is broken ie. so many 3 years graduates many with trivial RRA experience. That in fact we should go back to Foot and RRA to allow the RRA to be pooled to a smaller cohort.
Thanks for reading.
I may continue to correct small typoes after posting this. Unfortunately I could not post this with the images within the document.