- Joined
- Oct 4, 2017
- Messages
- 5,042
- Reaction score
- 9,841
inpt ; had to start emergent whole brain xrt

We can turn around an HA-WBRT plan in a few hours. I still do it as an inpatient. My dosimetrists and physicsts haven't killed me... Yet.
young pt w/ colon cancer, who wants aggressive care. Will have difficult time controlling gross disease.That's also brain (non-hippocampal) sparing WBRT. Or very, very large partial brain RT. Seems reasonable for a fraction or two before you convert them to IMRT, though I suppose.
If someone is inpatient for brain mets (unless like a rare new diagnosis, but then the role of 'emergent' WBRT makes me concerned) I usually don't do HA-WBRT.
Curious as to the clinical scenario in this patient.
We can turn around an HA-WBRT plan in a few hours. I still do it as an inpatient. My dosimetrists and physicsts haven't killed me... Yet.
young pt w/ colon cancer, who wants aggressive care. Will have difficult time controlling gross disease.
do you have standard beam arrangement/optimizations?We can turn around an HA-WBRT plan in a few hours. I still do it as an inpatient. My dosimetrists and physicsts haven't killed me... Yet.
do you have standard beam arrangement/optimizations?
OP could at least change the thread titleI hope Evilcore doesn't see this thread . . .
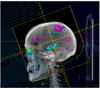
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes

I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
added an extra collimator sup and inf on hippocampus from picture and have mean dose of 5 Gy. Def blocking some brain, some of which is also not effectively treated with IMRT.I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
Emergent inpatient IMRT is not cool. Signals disdain for billers and physicists also.
Sent from my iPhone using Tapatalk
I hope Evilcore doesn't see this thread . . .
RickyScott were you able to meet all the hippocampal avoidance zone dose constraints from the NRG trial? I suppose the drawback of doing this is that you are probably sparing a lot more brain, which may be seeded with microscopic tumor, around the temporal lobes
beautifulinpt ; had to start emergent whole brain xrt
My theory on this is charge the IMRT plan that day 1. No consult, no devices, nothing. Just the plan. JUST THE PLAN. (And skip QA, for the physicists.)Emergent inpatient IMRT is not cool. Signals disdain for billers and physicists also.
Sent from my iPhone using Tapatalk
gangsta/inpt ; had to start emergent whole brain xrt
but you can SRS that later if needed right ?
And this is STILL chopping down a tree to get 7 apples. Yet creating less entropy than the original fieldsWell sure but then why not just shift your MLCs to do something like below? You can SRS that later if needed, right? Excuse the poor block angles - paint doesn't let me rotate at anything other than 90 degree angles.
Similar to breast-sparing mastectomies, the closest analogy in radiation oncology - brain sparing whole brain.
If you're going to partial brain, then just do partial brain (which I wouldn't). Again, it's fine for a treatment or two until you transition to IMRT, but would not do a full 10 treatment course like OP did.
View attachment 310479
")
beautiful
even better: just put a margin around the lesions and come in with the SRS a few fractions later.
).Kobe looked at Jordan and said “You’re pretty good but here’s where I can do it better.”Just did your lesion plus margin on a patient today due to mri delays! (although didn't include the edema

 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
Kobe looked at Jordan and said “You’re pretty good but here’s where I can do it better.”
Many times the patient with one brain met, or maybe two or two-plus etc, will have some sort of neuro compromise. And one will want to be getting the RT started right away, but WBRT is gauche, right? And "urgent," same-day SRS is kind of difficult. And there's some data that SRS upfront in neuro-compromised patients isn't the best. And maybe as Reaganite says you don't have an MRI yet...i know youve gone over it before, but what's your method again? thanks
I actually fully agree with this.Well sure but then why not just shift your MLCs to do something like below? You can SRS that later if needed, right? Excuse the poor block angles - paint doesn't let me rotate at anything other than 90 degree angles.
Similar to breast-sparing mastectomies, the closest analogy in radiation oncology - brain sparing whole brain.
If you're going to partial brain, then just do partial brain (which I wouldn't). Again, it's fine for a treatment or two until you transition to IMRT, but would not do a full 10 treatment course like OP did.
View attachment 310479