Anyone have a copy of the following that they are willing to share? Trying to save the $35 fee to
download.
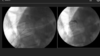
Radiofrequency ablation of splanchnic nerves for control of chronic abdominal pain
Kapural, Leonardo
Techniques in Regional Anesthesia & Pain Management , Volume 19 , Issue 3 , 138 - 142
download.
Radiofrequency ablation of splanchnic nerves for control of chronic abdominal pain
Kapural, Leonardo
Techniques in Regional Anesthesia & Pain Management , Volume 19 , Issue 3 , 138 - 142